



經常胸悶喘不過氣?看懂3個心肌梗塞警訊,提早預防就能保命
- 提早看懂警告訊號:心肌肌鈣蛋白飆高與心電圖異常,是心臟正在受損的鐵證,伴隨胸悶喘不過氣時必須立刻就醫。
- 把握黃金救援時間:確診急性阻塞後,盡快進行心導管介入治療或使用藥物打通血管,能有效保留最多的心臟功能。
- 長期穩定控制風險:術後務必按時服用 Aspirin 與 Statin 等藥物,配合飲食調整與體重管理,才能預防血管再次塞車。
心肌梗塞的發生,往往源自心臟肌肉長期缺氧與血液供需失衡,一旦抽血發現心肌肌鈣蛋白異常升高,就代表心臟細胞正在受損。提早看懂心電圖與抽血報告的警訊,並及時透過藥物或心導管介入治療,是挽救心臟功能的唯一關鍵。
金枝五十三歲,在巷子裡開了一家手工麵包店,每天凌晨四點就開始揉麵團、顧烤箱。她的雙手結實有力,一次可以搬起二十公斤的麵粉袋,自認身體比很多年輕人還硬朗。
最近兩個月,她發現每天下午出爐高峰期,彎腰從烤箱裡搬出烤盤的時候,胸口會悶悶的,像是有人用手掌壓住她的前胸。有時候那股悶感會延伸到左邊肩膀,甚至隱隱約約傳到後背。她一直以為是彎腰太久拉傷了肌肉,或是試吃太多剛出爐的可頌,胃食道逆流又犯了。

直到上週員工健檢,抽血報告回來,「高敏感度心肌肌鈣蛋白」那一欄出現了紅字。她拿去問藥局的藥師,藥師看了一眼,臉色立刻嚴肅起來:「這個你不能等,趕快去心臟科。」
門診時我看了她的心電圖,某幾個導程的 ST 段確實有微妙的變化。配合她描述的症狀——勞動時胸悶、放射到肩背、休息後緩解——這不是單純的腸胃問題,心臟正在發出求救訊號。
很多時候,心臟肌肉因為缺血而開始受傷,患者卻只覺得是疲倦或消化不良,完全沒想到事態的嚴重性。抽血報告上那些關於心臟的紅字,背後都隱藏著身體的求生機制,只要及早發現,我們都有機會逆轉局勢。今天就來聊聊,醫學上究竟怎麼判斷這些警告,以及你該如何保護這顆日夜跳動的馬達。
為什麼報告有紅字
抽血檢驗中的「心肌肌鈣蛋白」如果超標,就是心臟在告訴我們,它的細胞正在承受巨大的壓力甚至凋亡。這個蛋白質平常乖乖待在心臟肌肉細胞裡面,負責讓心臟順利收縮與放鬆。一旦心臟細胞因為缺氧而破裂死亡,這些蛋白質就會大量流進血液裡,讓檢驗儀器的警報器大聲作響。
為了讓大家更好理解這個複雜的醫學過程,我們可以把心臟想像成一座繁忙的城市。供應心臟養分的冠狀動脈,就像是運送物資的交通網絡,這條路的通暢與否,決定了這座城市的生死存亡。
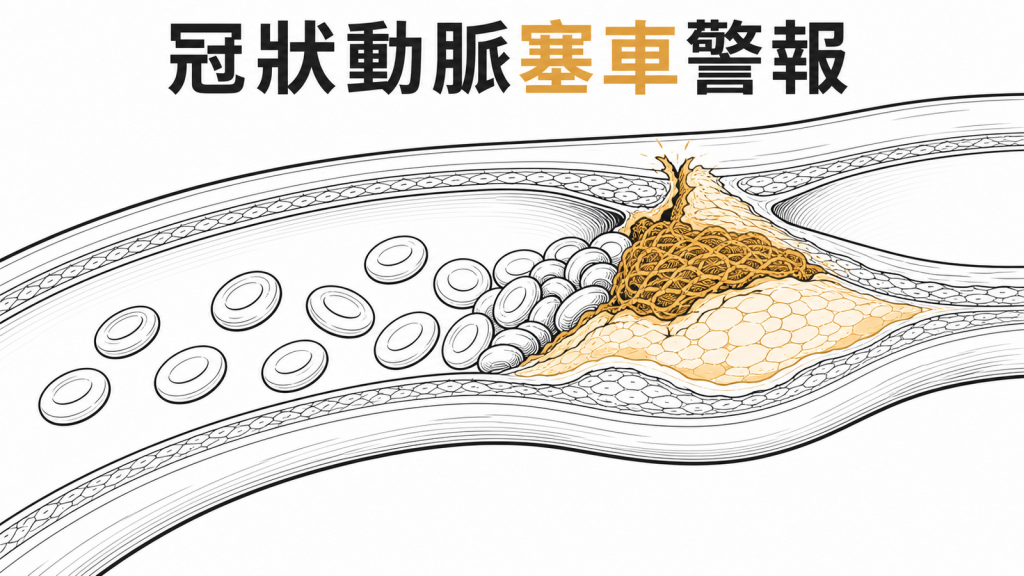
塞車的高速公路
心臟的肌肉需要豐富的氧氣才能不斷跳動,這全靠血管來穩定運送。當我們的血管壁因為膽固醇長期堆積,長出了厚厚的斑塊,原本寬敞的車道就會變得非常擁擠狹窄。某天這個斑塊突然破裂,血液中的血小板立刻衝過來結塊修補,瞬間引發嚴重的交通癱瘓。
這時候,載滿氧氣的紅血球根本過不去,後方等待救援的細胞等不到養分,就會開始慢慢餓死。這就是醫學上最典型的第一型心肌梗塞,主要是由急性血管栓塞所引起。當這些失去血液灌注的細胞大量死亡,血液中的發炎指標與破壞指數就會直線飆升。
幫浦過勞的馬達
有時候血管並沒有完全塞住,心臟卻依然發生了缺氧受損的狀況。你可以把心臟當成一顆抽水馬達,當你遇到嚴重感染、大出血或是極度焦慮時,身體會強迫這顆馬達用平常兩倍的速度狂轉。問題是,管線裡能提供的燃料根本不夠應付這種高速運轉,馬達最後就會因為過熱而燒壞。
這種因為「供給與需求極度不平衡」所造成的傷害,醫學上稱為第二型心肌梗塞。血管本身可能只有輕微狹窄,但因為身體其他部位的緊急狀況,迫使心臟超負荷工作。不管是哪一種原因,只要心臟細胞開始受損,我們就必須立刻啟動保護機制。
研究怎麼說?
很多民眾常常看著檢驗報告發愁,不知道這些專有名詞到底代表多嚴重的問題。醫學界對於心肌梗塞的診斷與治療,其實有一套非常嚴謹且不斷更新的國際標準。透過全球頂尖心臟科專家的研究,我們現在能用更精準的科學方法,揪出隱藏在數據背後的健康危機。
確診心臟受傷的黃金標準
單純的胸痛並不一定就是心肌梗塞,醫師需要綜合多項證據才能做出正確的判斷。根據國際心血管醫學會的共識,診斷的關鍵在於血液中的「心肌肌鈣蛋白」數值必須飆升超過正常人百分之九十九的上限值[1][4]。除了抽血數據之外,患者還必須伴隨明顯的心肌缺血症狀,像是劇烈胸悶、呼吸困難或是極度疲倦[1][4]。
有時候患者的感覺不一定準確,我們還需要依賴影像學的客觀證據來佐證。如果心電圖出現了新的缺血變化,或是超音波檢查發現某塊心臟肌肉突然失去活力,這都能確認心臟確實正在遭受攻擊[1][4]。這三個條件互相配合,就能大幅減少誤判的機率,讓真正需要急救的病人得到適當的資源。
心電圖顯示的兩種危機
一旦確認是心肌梗塞,急診醫師會立刻盯著心電圖,把病情分成兩種截然不同的等級。如果心電圖出現「ST段上升」,代表冠狀動脈已經完全被血栓塞死,心臟肌肉正在快速壞死[2][1][3]。這種狀況就像是主要幹道發生了嚴重走山,必須立刻出動怪手把道路搶通,否則後果不堪設想。
另一種情況則是「非ST段上升」,通常表示血管只有部分阻塞,或是旁邊還有一些微小的替代道路能勉強運送一點血液[2][1]。雖然這類病人的情況暫時沒有前者那麼致命,但仍然隨時可能惡化成完全阻塞。醫師會根據病人的風險高低,決定是要立刻安排手術,還是先用藥物穩定病情[2][3]。
五種不同的發病機制
你可能以為心肌梗塞都是吃太油、血管塞住造成的,其實醫學上把它細分成了五種不同的類型。第一型就是大家最熟悉的血管斑塊破裂引發血栓,第二型則是前面提過的供氧量與需求量嚴重失衡[1][2]。了解自己屬於哪一型非常重要,因為這直接關係到後續的治療方向。
第三型是指病人在還來不及抽血檢驗之前,就因為心臟停止而突然猝死,這種情況通常病情來得極為兇猛[1][2]。第四型與第五型則比較特殊,它們分別發生在心導管支架置放術以及冠狀動脈繞道手術的過程中[1][2]。任何手術都有潛在的風險,心臟血管的手術自然也可能對周邊組織造成一定程度的壓力與損傷。
搶時間的急救策略
面對急性心臟危機,時間就是保住心臟功能的絕對關鍵。對於完全阻塞的患者,第一線的首選治療是盡快進行心導管介入治療,用氣球把狹窄的地方撐開並放上支架[2][3]。如果病人所在的醫院沒有這項設備,醫師就會立刻注射血栓溶解劑,試圖用藥物把塞住血管的血塊化開[2][3]。
對於部分阻塞的患者,治療的重心會先放在防止血塊繼續擴大。醫師會給予強效的抗血小板藥物與抗凝血劑,同時密切觀察病人的疼痛指數與抽血變化[2][3]。只要及時穩住陣腳,配合後續的完整評估,多數病人都能平安度過最危險的急性期。
我需要進一步處理嗎?

| 指標狀況 | 建議行動 | 適合誰 | 追蹤時間 |
|---|---|---|---|
| 輕微胸悶、報告數值全數正常 | 調整飲食與作息,觀察症狀變化 | 偶爾感到疲倦的上班族 | 一年後例行健檢 |
| 僅心肌肌鈣蛋白輕微超標,無不適 | 回診請家醫科或心臟科評估其他原因 | 腎功能不佳或剛從重感冒痊癒者 | 三個月內回診抽血 |
| 三高數值亮紅燈,爬樓梯容易喘 | 安排心電圖或心臟超音波檢查 | 體重超標或有家族心血管病史者 | 一個月內至心臟科報到 |
| 劇烈胸痛蔓延至下巴或左肩,冒冷汗 | 立刻撥打一一九叫救護車 | 任何出現急性胸痛症狀的民眾 | 當下立刻就醫 |
有沒有副作用或風險?
醫學檢查和治療就像是一把雙面刃,能救人也可能伴隨一些意想不到的風險。抽血驗心肌肌鈣蛋白雖然很準確,但它也會出現令人虛驚一場的偽陽性結果。例如嚴重的腎臟功能衰竭、心肌炎或是敗血症,都會讓這個數值異常飆高,其實這時候血管並沒有真的塞住[1][6]。
如果單看抽血數據就貿然進行治療,反而可能對病人的身體造成不必要的負擔。這也是為什麼醫師總是不斷確認病人到底有沒有胸痛的症狀,並且反覆對比心電圖的變化[1][6]。仔細排除這些非缺血性的心肌損傷,才能避免走錯治療方向,把醫療資源用在刀口上。
至於治療方面,放支架和吃藥同樣需要承擔一定的副作用。打通血管的手術雖然成功率極高,但手術過程中仍有極低機率引發心律不整或血管受損。為了防止支架再次塞住,病人必須長期服用強效的抗血小板藥物,這會讓身體比較容易出現瘀青,甚至增加胃出血的風險。
即使有這些風險,比起心臟罷工帶來的致命威脅,接受正規治療的好處絕對遠大於壞處。醫師會根據每個人的年紀、肝腎功能和體重,精準調整藥物的劑量。只要患者願意好好配合醫囑,多數的副作用都能被控制在非常安全的範圍內。
醫師建議怎麼做?
心肌梗塞發作後,很多病人會以為出院就代表完全康復了。其實手術只是幫你把堵塞的馬路暫時清空,如果不改變生活習慣,這條路遲早會再次發生嚴重的坍方。想要真正遠離心臟危機,我們必須從日常生活的每一個小細節開始重新打底。
從吃下手減輕心臟負擔
飲食的選擇直接決定了血管裡會流動著清澈的泉水,還是濃稠的泥漿。建議多吃深綠色蔬菜、全穀類和富含優質蛋白質的魚肉,這些天然食物能減少身體的發炎反應。盡量避開加工肉品、反式脂肪和過多的鹽分,這能大幅降低血壓和膽固醇在血管壁上作怪的機會。
如果你的體重一直降不下來,適度的飲食控制配合醫療輔助會是很好的選擇。例如現在針對肥胖問題,醫師會評估是否適合使用像 Tirzepatide(猛健樂) 這類藥物來協助控制體重。猛健樂能有效減輕身體多餘的負擔,當體重下降後,心臟每天需要推動的血液量變少,自然就能跳得更輕鬆自如。
循序漸進的運動計畫
運動是讓心臟肌肉保持彈性最好的保養品,但千萬不能隨便逞強。對於剛做完心導管手術或是平時沒有運動習慣的人,建議從每天散步二十分鐘開始慢慢練習。感覺微微出汗、還能順暢聊天的程度,就是對心臟最友善的運動強度。
每一次運動前都必須做足十分鐘的暖身,讓身體的血管有時間慢慢擴張適應。冬天出門運動時也要特別注意保暖,因為冷空氣會讓血管瞬間收縮,增加心臟的壓力。如果運動中途出現任何頭暈或胸悶的感覺,請立刻停下來休息,絕對不要勉強自己撐完全程。
定期追蹤與按時服藥
回家後乖乖吃藥,是保護心臟免於二次傷害最基礎也最重要的一環。為了預防血栓再次形成並穩定血管斑塊,病人通常需要長期服用 Aspirin 以及 Statin 類的降膽固醇藥物[2][5]。這些藥物能幫血管內壁鋪上一層保護膜,讓後續的血液流通更加順暢無礙。
除此之外,醫師還會開立 Beta-blocker 或 ACE inhibitor 來減輕心臟的工作壓力並改善心衰竭的問題[2][5]。很多病患覺得症狀改善了就自己偷偷停藥,這往往是引發下一次嚴重復發的導火線。請按照醫師約定的時間乖乖回診,讓專業團隊幫你持續監測心臟的健康狀態。
常見誤解澄清
抽血數字正常,心臟就一定沒事嗎?
真相:心肌細胞受傷後,蛋白質釋放到血液中其實需要好幾個小時的時間。如果你才剛開始胸痛就衝去急診,第一次的抽血報告很可能完全正常,這很容易讓人掉以輕心。醫師通常會要求患者留在急診室觀察,幾個小時後再抽第二次血,這樣才能精準捕捉到數值攀升的關鍵時刻。
心肌梗塞只有胖子或老人家會得嗎?
真相:這幾年我們在診間看到越來越多三十幾歲的年輕人,因為突發性心肌梗塞被送進來。長期的工作壓力、熬夜抽菸、加上缺乏運動,這些不良習慣都會讓血管提早老化硬化。心臟保養從來就沒有年齡限制,只要你忽視身體的求救訊號,任何人都有可能成為下一個受害者。
裝了支架之後,心臟就完全康復了?
真相:放支架就像是請工人把塞滿垃圾的水管強行挖通,雖然水流暫時恢復了,但水管本身還是生鏽的。如果你繼續大魚大肉、不願意戒菸,新的垃圾很快又會把同一個地方塞住。手術只是一個讓你重新開始的契機,後續的保養與長期的藥物控制,才是決定這支架能用多久的關鍵。
只有胸痛才是心肌梗塞的症狀嗎?
真相:很多女性或是糖尿病患者發病時,根本不會感覺到標準的胸痛。他們可能會出現難以解釋的胃痛、呼吸急促、下巴痠痛,甚至是極度的疲倦感。這些不典型的症狀經常被誤以為是太累或是感冒,錯失了第一時間就醫搶救的黃金空檔。
重點整理
- 提早看懂警告訊號:心肌肌鈣蛋白飆高與心電圖異常,是心臟正在受損的鐵證,伴隨胸悶喘不過氣時必須立刻就醫。
- 把握黃金救援時間:確診急性阻塞後,盡快進行心導管介入治療或使用藥物打通血管,能有效保留最多的心臟功能。
- 長期穩定控制風險:術後務必按時服用 Aspirin 與 Statin 等藥物,配合飲食調整與體重管理,才能預防血管再次塞車。
參考文獻
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction (2018). Journal of the American College of Cardiology. 2018;72(18):2231-2264. DOI: 10.1016/j.jacc.2018.08.1038
- Anderson JL, Morrow DA. Acute Myocardial Infarction. The New England Journal of Medicine. 2017;376(21):2053-2064. DOI: 10.1056/NEJMra1606915
- Reed GW, Rossi JE, Cannon CP. Acute Myocardial Infarction. Lancet. 2017;389(10065):197-210. DOI: 10.1016/S0140-6736(16)30677-8
- Thygesen K, Alpert JS, White HD, et al. Universal Definition of Myocardial Infarction. Journal of the American College of Cardiology. 2007;50(22):2173-95. DOI: 10.1016/j.jacc.2007.09.011
- Lu L, Liu M, Sun R, Zheng Y, Zhang P. Myocardial Infarction: Symptoms and Treatments. Cell Biochemistry and Biophysics. 2015;72(3):865-7. DOI: 10.1007/s12013-015-0553-4
- DeFilippis AP, Chapman AR, Mills NL, et al. Assessment and Treatment of Patients With Type 2 Myocardial Infarction and Acute Nonischemic Myocardial Injury. Circulation. 2019;140(20):1661-1678. DOI: 10.1161/CIRCULATIONAHA.119.040631
醫療免責聲明
本文內容僅供衛教參考,不構成個人醫療建議、診斷或治療方案。任何健康問題請諮詢您的主治醫師或合格醫療專業人員。博田國際健康管理中心對依據本文內容所做之決定不承擔任何責任。
最後審閱日期:・作者:黃柏誠醫師